Only 25 more days of Leukemia treatment!
February 2nd, 2024

Acute Promyleocytic Leukemia sucks, but as sucky things go, this hasn’t been so bad.
Today we had another confab with the Leukemia “fellow,” Dr. Premji, this one in person down in Rochester. She’s very cool, and we’re impressed. Alan’s been getting the best of care imaginable. He’s in the final “cycle” which will be winding up near month’s end. WHAT A RELIEF!!!

We got a look at what’s next, after finishing this EIGHT MONTH LONG round of daily treatment. It’s on a rotating basis back and forth between one cycle with 2 weeks of IV arsenic (arsenic on weekdays) and oral ATRA everyday and then 2 weeks of arsenic only (on weekdays); and the other cycle of 2 weeks of oral ATRA only and then 2 weeks off both. Eight alternating cycles, beginning in July after his June 23rd discharge, and at long last, the last infusion is February 27. TWENTY FIVE DAYS TO GO!
After treatment ends, Dr. Premji said it would be a few months until Alan’s immune system builds up after this extreme treatment, so probably June, but with COVID running rampant again, it’s a good time to be masking and isolating.
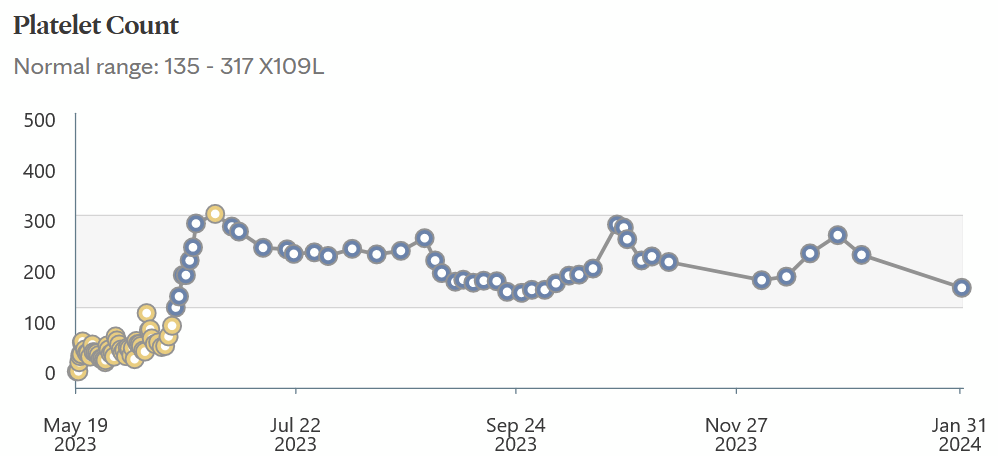
Platelets always go down a bit during an arsenic cycle, so no worries, they’ll bounce back! And what an improvement after that initial level of NINE (9) on admission. That rather freaked the doctors out! He’s been in remission since some time in that first blue spike “induction” phase ended, technically in remission on discharge June 23. Outpatient, it’s the “consolidation” phase (no idea why it’s called that), and it’s soon completed.
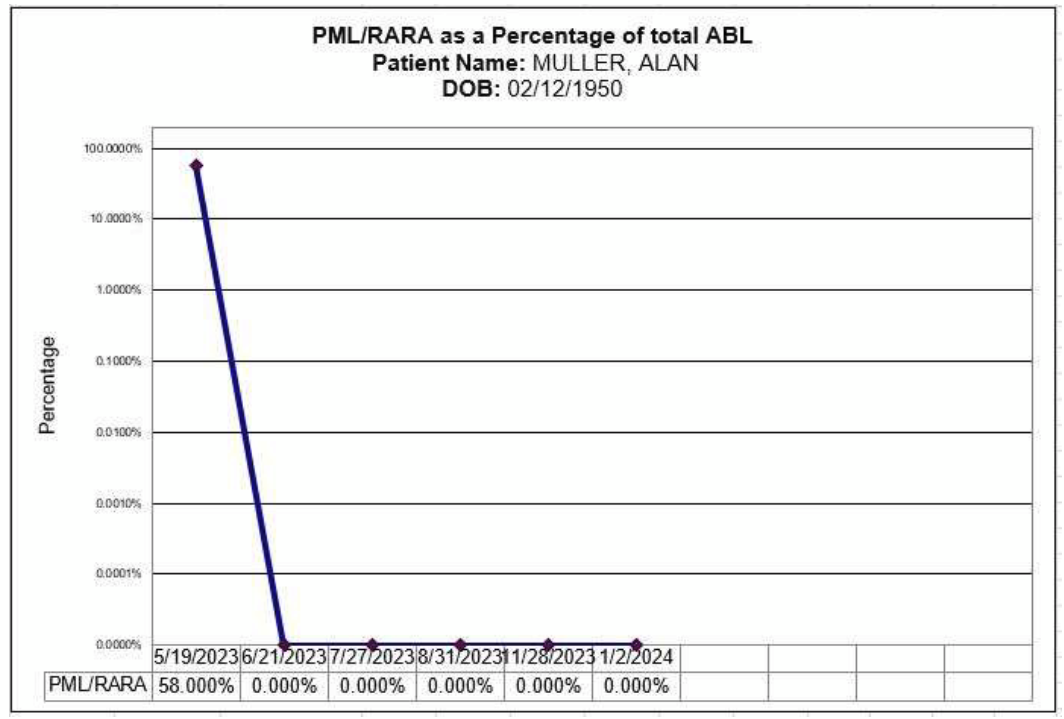
We’re still waiting on this month’s PML/RARa, should be back in a few days, but here’s verification of the good news, the nasty cells are down to ZERO and have been since early on:
After our March visit, he’ll be scheduled for a visit every 3 months. She said he’s been doing exceptionally well, far better than most, with almost no side effects, mindful that this is not chemo. It’s “treatment,” and always the APL treatment side effects of this are less, not at all debilitating or even uncomfortable, just some weird stuff, occasional headaches, skin falling off!!! We’ve only had one real bump in the road, pneumonia in October, with quick recovery. WHEW!
And after getting back from Rochester, another arsenic infusion today in Red Wing… Can’t wait until we’re done with these Rochester treks, and constant appointments here too, though now at least we know where we’re going in the Rochester tunnels, elevators, and we have quite a few “get out of jail free” cards for the parking lot. Red Wing always takes a long time to get the infusions going, but at least he can get them done here, that helps a lot.
Alan said he’d like another picnic at the Gonda building entrance…

He had to see his doggy, and Mayo wouldn’t let Sadie in, so when weather was good, we had an Indian feast at the door — veggie korma and palak paneer, pakora with lots of coriander chutney, and garlic naan of course. Frankly, that month-plus in the hospital was a rough time I’d rather not relive!
Yup, I’m counting the days until this is OVER! Last arsenic dose, arsenic and ATRA treatment ENDS on February 27th. Another bone marrow biopsy a week later, and meet for our “exit interview” after that.
TWENTY FIVE DAYS TO GO!!!
Muller update – APL still sucks!
June 2nd, 2023
UPDATE: It’s been two weeks now. Alan is settled into room 9-415 in Eisenberg in Mayo’s Methodist campus . He’s still short on platelets and getting a refrigerated batch right now. He IS feeling MUCH better, no longer utterly worn down, no longer bruising all over and the earlier bruises are slowly fading away. Not long ago, Acute Promyelocytic Leukemia was a death sentence, and no longer. Things have changed in leukemia world, and the medical care at Mayo is top notch. I’m particularly impressed with the nurses who are ON this, with multiple infusions going, platelets, arsenic, and antibiotics. As of yesterday (?) antibiotics are done and his hand is healing, almost done, no longer infected.
And yes, arsenic. He’s on half doses and that will be increasing sometime next week. For APL, the treatment that apparently works is ATRA, which is a Vitamin A derivative (weird, huh?), and arsenic (even weirder!). I’d wondered about treating dog’s heartworm with arsenic, particularly when our Kady-Kate lost her marbles and spent her days staring into space, but I’d checked with three vets and none knew anything about potential of impact of arsenic on cognition. We’ll see!

Anyway, Alan’s doing well, now has a PIC line, making the infusions easier, and they’d said in particular they want it in for arsenic infusions. OK, whatever, here we go! He’s up and about, making regular trips to the hospital library down in the basement, bringing back a load of books each time, and it looks like I’m going to have to bring in a bookshelf!
Since he can go hang out downstairs in the library for an hour or more, I’m trying to finagle a picnic with Little Sadie. Alan really misses his doggie, and there’s a good driveway where we could do a pick-up!

Acute Promyelocytic Leukemia SUCKS
May 20th, 2023

Well this was quite a surprise. Alan was feeling tired for a couple of weeks and had a pretty large bruise on upper hip, to over a couple days larges bruises all over, and OMFD, it’s Acute Promyelocytic Leukemia. I’d had an inkling of CLL after taking photos of the bruises to send to Mayo here in RW, and hitting google, so I was pushing him hard to get in fast, and thankfully he did. Platelets were alarmingly low from Nurse Practitioner’s rather wide-eyed response, which was to get us to the ER, STAT. We were there most of the day, and then after 2nd big batch of lab results came in, he was rushed to Mayo about 4:30. He’ll be at Mayo now for 3-4 weeks, started chemo immediately, and platelets, as his were nearly zero.
Despite 2nd shift, they were on it right away, the nurses and aids were very attentive, and the Nurse Practitioner on that evening was so articulate about what’s going on. Treatment plan is to start aggressively, pretty much as explained in the link below, and see what happens.
Alan’s just getting settled in, and he’s not sure if he wants visitors yet — feel free to message him or text or call.
Treatment of Acute Promyelocytic Leukemia
It seems APL hits middle-aged folks with average age in the 40s, but for seniors it’s the leukemia of choice. The standard treatment before this regimen (Mayo has links to various study’s participant recruitment!) had some long-term side effects, and apparently this is better. I was wondering about treating with arsenic, remembering Kady who was treated for heartworm with arsenic and lost her marbles, and I’ve asked a few vets about long term impacts of arsenic and neither I’ve asked knew anything about it, and google knows nothing. Alan’s deemed “low risk” because it was caught fairly soon and his white blood count is below the “10k” magic number.
I’d learned some about leukemia when dealing with magnetic fields associated with transmission lines, argued need for regulatory action before the appellate court 20 years ago, but no, earlier bad decision affirmed… And I’ve long known of cancer clusters, and the increases in childhood leukemia in certain scenarios. Environmental impacts have long been ignored, and causation, that ephemeral target, has not yet been established for so many likely agents responsible.
Delaware is a waste dump of the U.S., polluted in so many ways, and Alan’s horror stories make me wonder why anyone wold live there. I’ve thought about Alan’s cancer risk having lived next to 3 nuclear reactors…

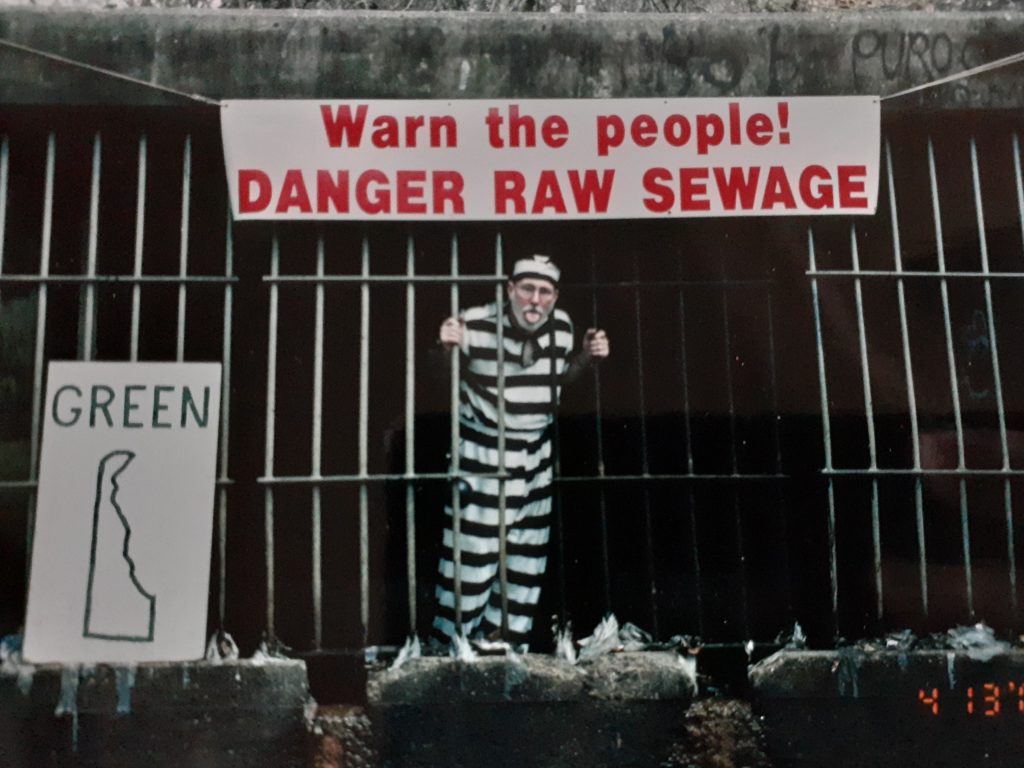
… probably downwind of TMI, and for sure downwind from the Delaware refinery that spews all over everyone in Delaware City, Port Penn, and beyond. Somebody asked, “Who’s Alan?” Just google Green Delaware! For decades Alan worked to improve Delaware, from exposing the ractice of dumping raw sewage into the Brandywine River, and being arrested for putting a “Danger Raw Sewage” sign at the outflow:


Busted again at the legislature when public participation was prohibited — with John Kowalko, later STATE REP. John Kowalko, who just retired:

And then in 2007 starting work against Minnesota incinerators, when he got a call out of the blue from someone in St. Paul wanting help on the Rock Tenn incinerator. He’d worked for DuPont as consultant, and part of that was worldwide promotion of incinerators, and he learned a LOT about what incinerators inflicted on those breathing nearby. The call from St. Paul came in when I was out there on my 2nd trip to Port Penn, and they’d wanted him to come out for a Neighbors Against the Burner gathering on the date we’d planned to get back to Red Wing, all just too coincidental! That was the start of a long collaboration with Neighbors Against the Burner and challenging Rock Tenn, the E. Phillips “Eco-Crapper” burner later tried in Rockford and stopped there too; expansion of HERC, and pushing to shut down City of Red Wing’s incinerator, now closed:


So back to Acute Promyelocytic Leukemia — need to get on the road. Suffice it to say, I’ve started on my “research.” Don’t cringe, beyond google, DOH! Years back when I was doing radio, I’d done a program. on bendictin, and another on DES, which was used with wild abandon and without informed consent on Native women. I was working at HCMC and using their medical library a LOT, and in the short time I worked at Bone Marrow Transplant I learned a lot I didn’t really want to know, that was a difficult station with so many babies and young children… I also am well aware that much has changed over the last 40 years, so there’s a lot of reading and evaluating to do to catch up.
A few available things, hope to tap into some deeper sources, but these are interesting:
How retinoic acid and arsenic transformed acute promyelocytic leukemia therapy