Only 25 more days of Leukemia treatment!
February 2nd, 2024

Acute Promyleocytic Leukemia sucks, but as sucky things go, this hasn’t been so bad.
Today we had another confab with the Leukemia “fellow,” Dr. Premji, this one in person down in Rochester. She’s very cool, and we’re impressed. Alan’s been getting the best of care imaginable. He’s in the final “cycle” which will be winding up near month’s end. WHAT A RELIEF!!!

We got a look at what’s next, after finishing this EIGHT MONTH LONG round of daily treatment. It’s on a rotating basis back and forth between one cycle with 2 weeks of IV arsenic (arsenic on weekdays) and oral ATRA everyday and then 2 weeks of arsenic only (on weekdays); and the other cycle of 2 weeks of oral ATRA only and then 2 weeks off both. Eight alternating cycles, beginning in July after his June 23rd discharge, and at long last, the last infusion is February 27. TWENTY FIVE DAYS TO GO!
After treatment ends, Dr. Premji said it would be a few months until Alan’s immune system builds up after this extreme treatment, so probably June, but with COVID running rampant again, it’s a good time to be masking and isolating.
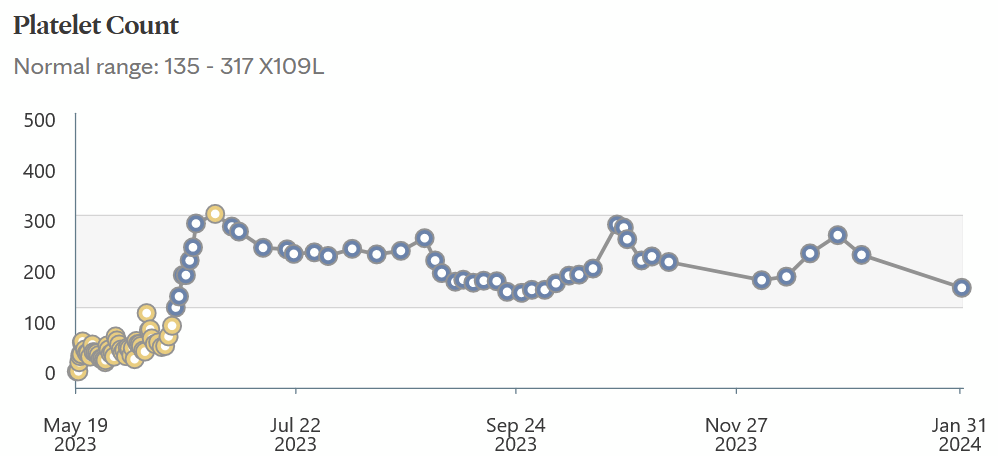
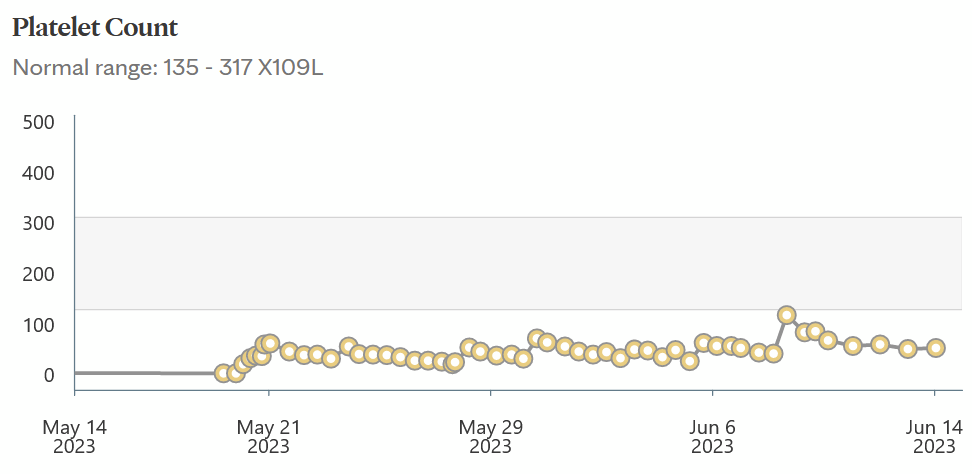
Platelets always go down a bit during an arsenic cycle, so no worries, they’ll bounce back! And what an improvement after that initial level of NINE (9) on admission. That rather freaked the doctors out! He’s been in remission since some time in that first blue spike “induction” phase ended, technically in remission on discharge June 23. Outpatient, it’s the “consolidation” phase (no idea why it’s called that), and it’s soon completed.
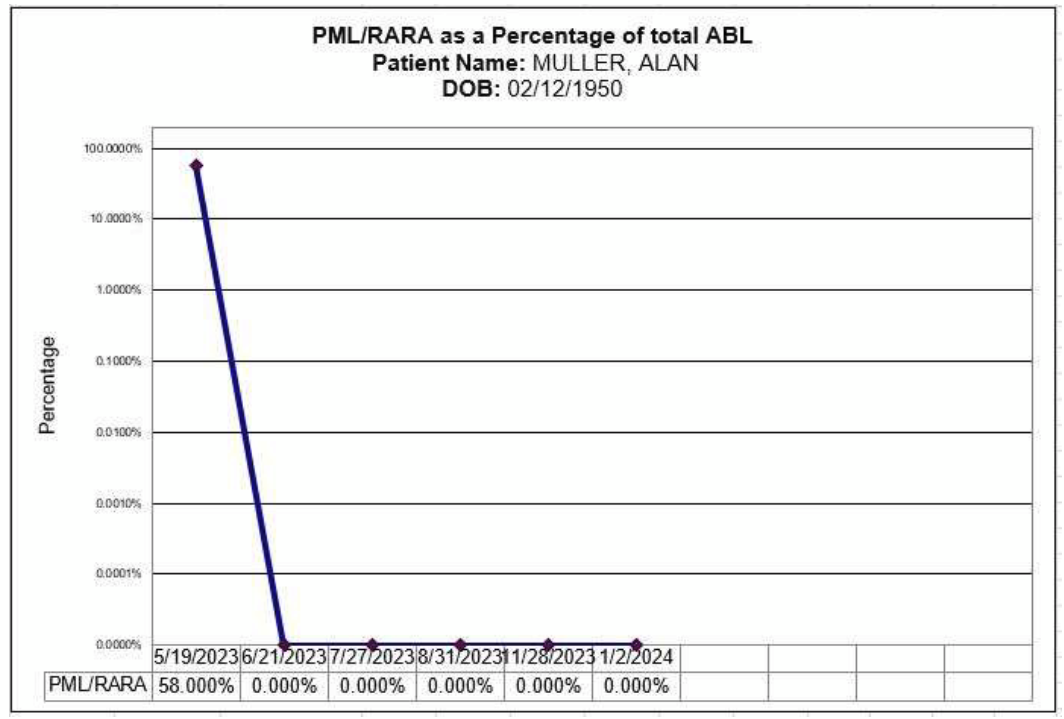
We’re still waiting on this month’s PML/RARa, should be back in a few days, but here’s verification of the good news, the nasty cells are down to ZERO and have been since early on:
After our March visit, he’ll be scheduled for a visit every 3 months. She said he’s been doing exceptionally well, far better than most, with almost no side effects, mindful that this is not chemo. It’s “treatment,” and always the APL treatment side effects of this are less, not at all debilitating or even uncomfortable, just some weird stuff, occasional headaches, skin falling off!!! We’ve only had one real bump in the road, pneumonia in October, with quick recovery. WHEW!
And after getting back from Rochester, another arsenic infusion today in Red Wing… Can’t wait until we’re done with these Rochester treks, and constant appointments here too, though now at least we know where we’re going in the Rochester tunnels, elevators, and we have quite a few “get out of jail free” cards for the parking lot. Red Wing always takes a long time to get the infusions going, but at least he can get them done here, that helps a lot.
Alan said he’d like another picnic at the Gonda building entrance…

He had to see his doggy, and Mayo wouldn’t let Sadie in, so when weather was good, we had an Indian feast at the door — veggie korma and palak paneer, pakora with lots of coriander chutney, and garlic naan of course. Frankly, that month-plus in the hospital was a rough time I’d rather not relive!
Yup, I’m counting the days until this is OVER! Last arsenic dose, arsenic and ATRA treatment ENDS on February 27th. Another bone marrow biopsy a week later, and meet for our “exit interview” after that.
TWENTY FIVE DAYS TO GO!!!
Camping in the midst of leukemia treatment?
July 2nd, 2023

I be bummin’ over having to cancel two long awaited and intensely planned and saved and paid for trips, though clearly Alan’s Acute Promyelocytic Leukemia is even more of a bummer. And the good news is he’s out of the hospital, feeling good, and not wiped out by the treatments, AATRA and arseic treatments that will be ongoing until ? February probably.
The ATRA is just oral meds, and it’s not debilitating, no discomfort, apparently no side effects. Treatment alternates between 2 weeks of daily ATRA at home, and then 2 weeks of daily arsenic at RW Mayo, so we’re going to try camping on an ATRA time, and see how that goes. Then, as we get into the groove, perhaps more, though for sure we can’t afford long trips, the side effects of costs ARE debilitating.
Took the plunge and booked a site.

Haven’t stayed in Frontenac for a LONG time. Site 32, last September:

And spur of the moment over Xmas 2021 in the hybrid, that was a hoot:

Close to home, and short time, should be workable. We shall see…
Great news from Mayo!
June 17th, 2023
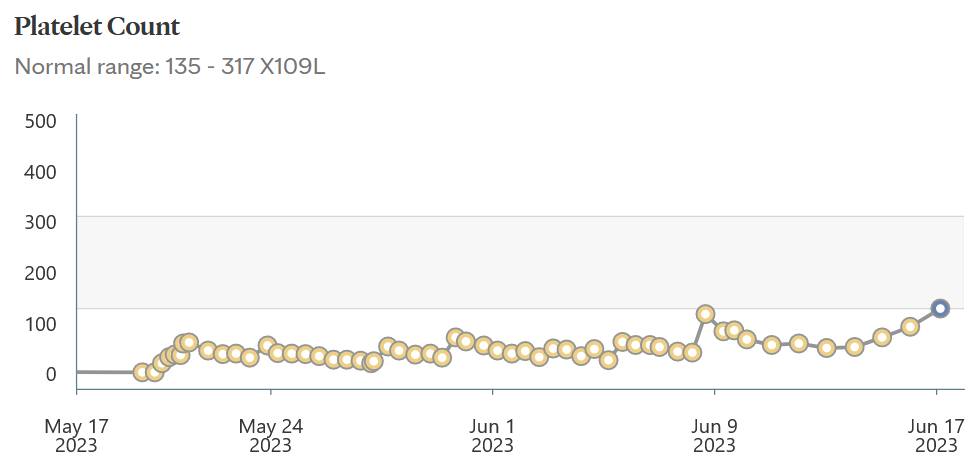
Today’s platelet count hit NORMAL! 135! That’s up from 9, yes, NINE, on admission.
This is such good news, heaving a sigh of relief. When the doctors say Alan is doing “better than expected” this is a most positive spin on that statement!
Muller update, LIVE from Mayo!
June 14th, 2023

Above is a quilt made and gifted by Marilyn Tkachuk, intensely detailed, easily hundreds of hours of work. Just WOW. Marilyn and Tilton have been in to visit, and Marilyn’s been there, has been to Rochester lately for testing, and knows too well how life-changing a cancer diagnosis, chemo, and this “new normal” can be. Her support means so much… Thank you all for inquiries, visits, calls, and care packages, he appreciates that y’all are thinking of him. I’ll keep “updates” on the calendar so you’ll have some idea what’s going on. Lately, it’s just more of the same, B-O-R-I-N-G! But that’s good news in hematology!
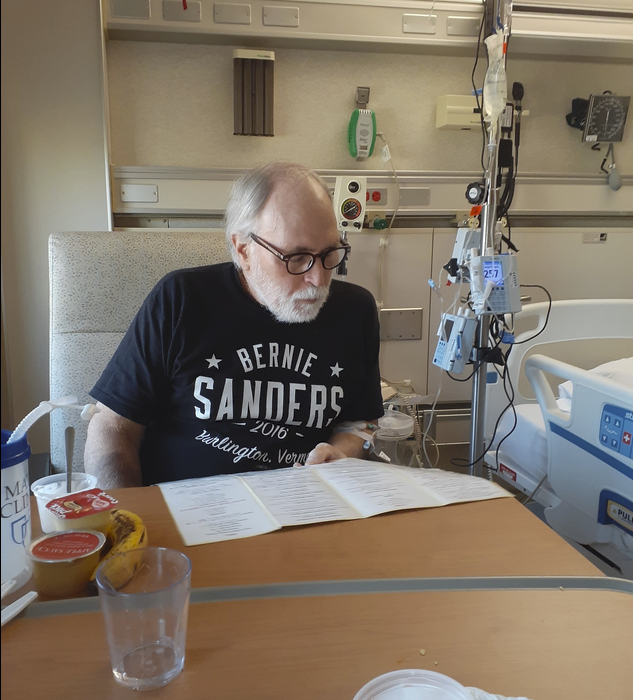
Alan’s still in Mayo, Methodist campus, Eisenberg 9-416 (3rd room so far). If you’d like to visit, do give him a call to check his schedule, he’s in and out, poked and prodded often every day. (302) 299-8638.
Alan’s stabilized, doing well, Drs. say “you’re doing better than expected” and yet needs to be in another 3 weeks before he’s discharged. After discharge, there’s DAILY chemo for SEVEN MONTHS, alternating months between a month of oral ATRA (vitamin A derivative) and a month of IV arsenic(yes, that arsenic) at some Mayo facility, and hopefully NOT Rochester (that’s a 3,000 mile a month journey). Back and forth, month ATRA, month arsenic, seven months, so likely through January, into February? I hope by Alan’s birthday it’ll be “Happy Birthday to you, you’re done with CHEM-O.” Until then, onward with treatment and figuring out what life will be like going forward.
Platelet count has been a major concern, that was the trigger that caught our attention, because low platelet count means bleeding, and suddenly he was covered in bruises. Bleeding can start spontaneously or with a bump, and doesn’t clot. A fall can be deadly. When he was in the clinic, and then the ER, he had a platelet count of 9. Yes, NINE! They were popping their eyeballs in shock, got him in the ER stat, and they wouldn’t even let me drive him to Rochester, hence an ambulance with lights and siren.
He’s got a PICC line in now, getting regular platelet infusions, and it seems to be a peak and trough, with peak raising it, and trough then not so low, another peak, and then not as low, so he’s above the crisis point, but no where near normal, more like half of normal, but not NINE! They want to keep platelets over 50. Bruising is fading, and no new ones, so PROGRESS is visible.
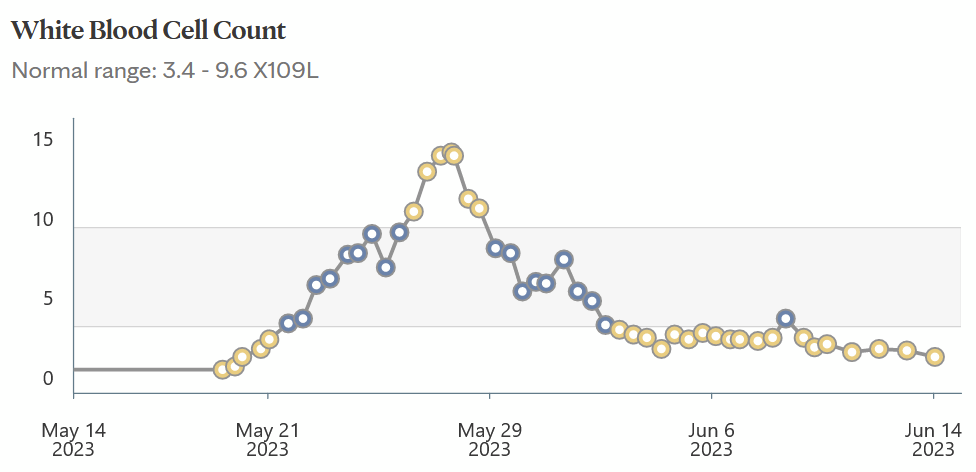
White blood count is an issue too, as we’ve been told that what’s happening is that his white blood cells aren’t “maturing” and with the chemo, they’re being released when not read due to the chemo, and too many too soon triggers, or is, differentiation syndrome:

That means there’s a balance of quick release that signals the release of the deadly stuff, too many WBCs v. keeping them in, keeping it low, so there’s daily testing and monitoring, and adjusting the teeter-totter.

You can see the sharp peak exactly 2 weeks after starting treatment, and, whew, then a sharp drop, lowering, I think, to where it should be.
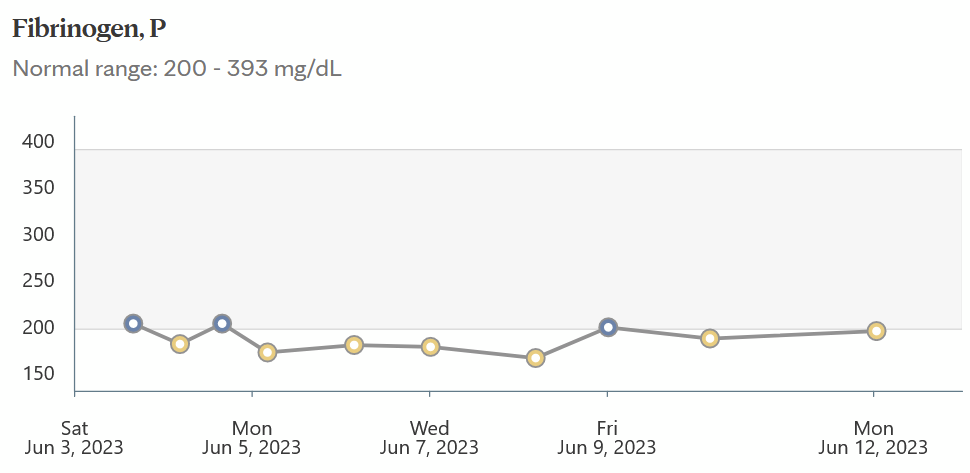
Fibrinogen is also an issue, but that seems stable:
I’m posting these updates, trying for weekly, but missed last week’s (!), because there aren’t enough hours in the day. It’s hard to explain the details over and over, so these updates are the nutshell. It’s a steep learning curve with so many variables, and IT’S SUCH LONG TREATMENT. We’ve been told that 90% get through this “induction” phase, which is the hospitalization and stabilization, and it seems he’s in that 90%. They’re constantly monitoring him, sucking blood out of him like the Minnesota State Bird.

The new normal is a new part-time to full-time job, taking up even more head space than actual time doing all that needs to be done, an extremely high band-width endeavor on this end, and I’d guess even more so for Alan, though he’s bored shit-less there, spending a lot of time at the hospital library now that he can roam the halls. TV is against his religion, though I hope he got to see what reporting there was of Trump’s arraignment.
We’ve had a picnic with Sadie, because he SO misses his dog (plus there’s real food in Rochester, in RW, there’s little to choose from), and need to do another soon:
Sadie never smiles, but look how happy she is to see Alan!
Onward…
Muller update – APL still sucks!
June 2nd, 2023
UPDATE: It’s been two weeks now. Alan is settled into room 9-415 in Eisenberg in Mayo’s Methodist campus . He’s still short on platelets and getting a refrigerated batch right now. He IS feeling MUCH better, no longer utterly worn down, no longer bruising all over and the earlier bruises are slowly fading away. Not long ago, Acute Promyelocytic Leukemia was a death sentence, and no longer. Things have changed in leukemia world, and the medical care at Mayo is top notch. I’m particularly impressed with the nurses who are ON this, with multiple infusions going, platelets, arsenic, and antibiotics. As of yesterday (?) antibiotics are done and his hand is healing, almost done, no longer infected.
And yes, arsenic. He’s on half doses and that will be increasing sometime next week. For APL, the treatment that apparently works is ATRA, which is a Vitamin A derivative (weird, huh?), and arsenic (even weirder!). I’d wondered about treating dog’s heartworm with arsenic, particularly when our Kady-Kate lost her marbles and spent her days staring into space, but I’d checked with three vets and none knew anything about potential of impact of arsenic on cognition. We’ll see!

Anyway, Alan’s doing well, now has a PIC line, making the infusions easier, and they’d said in particular they want it in for arsenic infusions. OK, whatever, here we go! He’s up and about, making regular trips to the hospital library down in the basement, bringing back a load of books each time, and it looks like I’m going to have to bring in a bookshelf!
Since he can go hang out downstairs in the library for an hour or more, I’m trying to finagle a picnic with Little Sadie. Alan really misses his doggie, and there’s a good driveway where we could do a pick-up!
